ABOUT AfriMedico私たちについて
医薬品の提供を通じて
アフリカの全ての人々へ
当たり前の医療を届けたい。
アフリカでは医療資源そのものが不足しており、
今私たちが当たり前のように受けている皆保険制度も存在しません。
インフラの不整備等により病院や薬局までのアクセスが悪い、
病院までアクセスできても受診までの待ち時間が長い、
受診料が高いといった問題があり、
その結果、病気にかかっても容易に医療サービスを受けられず、
その間に、病気が重症化して、最悪の場合死に至ることもあります。
このような状況を少しでも改善するために、
日本発祥の置き薬の仕組みで
アフリカのすべての人々健康と笑顔を届けたい、
私たちはこのように考え、AfriMedicoを結成しました。
MISSION
医療を通じて、
アフリカと日本をつなぎ、
健康と笑顔を届ける。
300年以上前の江戸時代から続く日本発祥の「置き薬」の仕組みを現代版に置き換え、
医療アクセスが行き届かないアフリカ農村部へ薬を届けています。

アフリカの人々の
健康への寄与

日本製薬業界の
更なる発展
WHAT WE DO
日本の伝統的な
「富山の置き薬(配置薬)」の
仕組みを現代版に置き換え、
アフリカに広めるべく
活動しています。
置き薬とは、家庭や公共の場(学校や企業など)に基本的な薬剤のセットを置いておくサービスです。AfriMeicoが支援する置き薬の普及活動では、薬箱の設置には費用がかからず、病気や怪我で置き薬を使ったときにだけ、使用した分の費用を患者さんが払います。 この仕組みによって、患者さんは遠い病院に行き、長い待ち時間を過ごす必要が無くなります。必要な時に必要な医薬品を使用できるので、置き薬は「ホームドクター」のようなものと言ってもよいでしょう。 既に置き薬を取り入れている海外の事例では、病気の重症化を防いだり、人々の医療に関する知識を増やしたりするといった形で健康に寄与しています。

Activity 1置き薬事業
置き薬について配置薬は江戸時代の富山の薬売りから始まり、現在まで続いている一般用医薬品の販売方法の1つです。配置薬は国民皆保険制度が整うまで、我が国において大きく発展し、最も普及していたころには近畿地方の約80%の家庭に配置薬があったとの報告もあります。配置薬の中には風邪薬・消毒薬・頭痛薬・下痢止めなど繁用医薬品が含まれています。消費者は「先用後利」の理念に基づき、必要な時に必要な医薬品を使用し、代金は使用した分のみを負担します。現在、配置薬モデルはアジアを中心に様々な国々に輸出されており、例えばモンゴルでは国策として配置薬の整備がなされています。
close日本発祥の伝統的な医療モデルの1つである”置き薬“を現代版に置き換えてアフリカに広めるべく活動しています。とくに都市から離れた農村部の各家庭に対して、置き薬を紹介し、より良い医療がより多くの家庭に届くことを目的に活動をしています。

Activity 2医療教育事業
アフリカ現地でイベントやセミナー、患者さん向けの医療教育冊子等の提供を通じて薬の正しい使い方や病気の予防、治療の方法をより多くの方に知って頂けるよう活動しています。置き薬の紹介だけでなく、より多くの患者さんに病気のことをきちんと知ってもらえる機会を提供しています。

Activity 3研究事業
アフリカの一般家庭ではどのような医薬品が必要とされているのか、医療アクセスが行き届かない家庭に置き薬がどう有用なのか、独自のネットワークを用いて研究活動を推進しています。医療アクセスとセルフメディケーションの促進に向けて、タンザニアのムヒンビリ国立大学と提携し共同研究を進めています。

Activity 4広報事業
日本の皆さんにアフリカの医療環境をもっと知ってもらいたい、アフリカにはどのような病気が多く、どのような薬剤が求められているのか、私たちが草の根で活動を進める中で学んできた知見やアフリカの現況をより多くの方々へお伝えするために定期的にセミナーや勉強会等のイベントを開催しています。

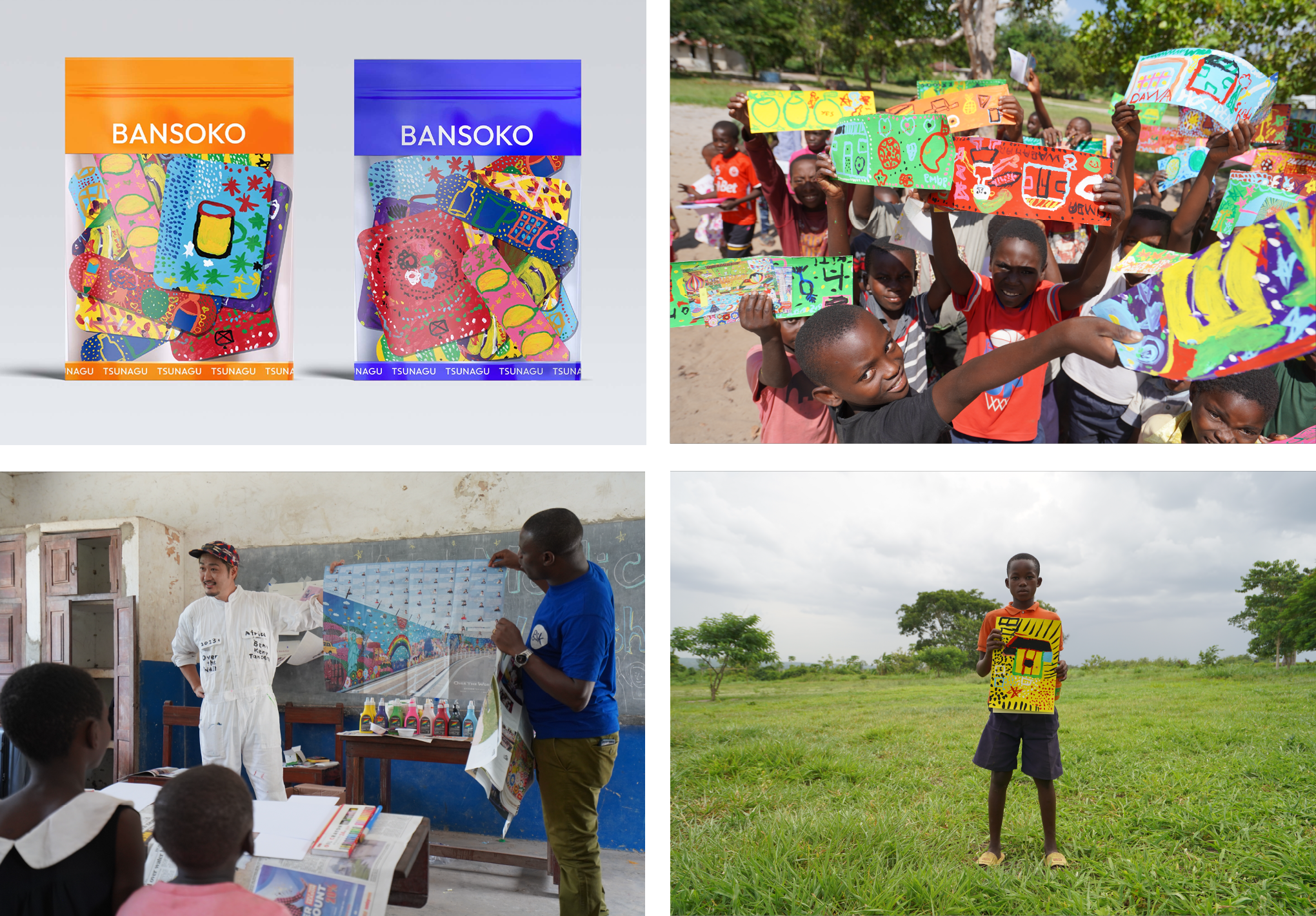
Activity 5新規事業
AfriMedico TSUNAGUアフリカと日本をつなぐというミッションに基づき、アフリカの文化や価値を、未来を担う日本の子ども達に知ってもらう新しい事業へ取り組んでいます。様々なパートナー様とのコラボレーションを通じた本事業で得られる日本国内での事業収益を全てアフリカの置き薬事業へ還元しています